
 , 王明月, Wang Mingyue
, 王明月, Wang Mingyue【目的】以用户感知价值视角, 构建一套集“用户、信息技术、医院服务人员”于一体的交互影响式医疗信息服务评价体系。【方法】提出基于主成分分析法统计指标成分占比和实现指标筛选, 灰色聚类方法确定指标关联矩阵和临界值且实现指标优化, 组合方法的搭建可测评医疗信息服务评价体系质量。【结果】评价指标体系共有9类58项指标为, 且服务价值维度权重比例最大为0.2059, 风险成本维度权重比例最小为0.0405。【局限】量表问卷数据样本范围较小, 指标分值由少数专家打分确定, 具有一定程度上的主观性。【结论】贯穿“用户、信息技术、医护人员”三元一体的评价体系能够在理论上为医院医疗信息服务建设、规划与管理提供决策依据, 在实践应用上提高医院医疗信息服务的水平和用户的体验满意度。
[Objective] This paper constructs an interactive impact assessment system for medical information services that integrates users, information technology and hospital staff, from the perspective of user perceived value. [Methods] The proportion of statistical indicators and the screening of indicators are proposed based on principal component analysis, the Grey clustering method determines the index correlation matrix and the critical value in order to achieving the index optimization. Establishment of combination method can evaluate the quality of medical information service evaluation system. [Results] The evaluation index system includes 58 indicators and can be divided into 9 categories. The maximum weight proportion of service value dimension is 0.2059, and the minimum weight proportion of risk cost dimension is 0.0405. [Limitations] The scale of the questionnaire data is small. The index scores are determined by a few experts and have a certain degree of subjectivity. [Conclusions] The proposed evaluation system can theoretically provide decision-making basis for hospital medical information service construction, planning and management, and improve the level of hospital medical information service and user's experience satisfaction degree in practical application.
近年, 在医疗信息化发展进程中, 医疗信息服务为用户(包含患者与亚健康人群)提供便利条件, 美国、德国与英国等多数发达国家在以信息技术处理手段为基础的医疗信息服务发展方面已取得较大进展[1], 其相关的医疗信息服务体系和水准已发展到一个较新阶段。信息手段的医疗服务极大地改变了传统医疗服务模式, 有效地改善了医疗过程中用户、医院及服务人员所面临的就医复杂、处理率低、医患沟通不及时的弊端[2]。此外, 用户也可通过信息化手段更好地了解医院、医生和诊疗过程, 促使其建立对医院和医生的信任感与信心, 改进医生与用户的紧张关系, 同时极大地促进用户参与到医疗过程中。因此相关学者聚焦于医疗信息服务研究, 进而提升医疗信息服务水平, 以更好地为用户服务。
医疗信息服务意指信息技术手段下, 医院所提供的一种医疗方面的服务[3]。而医疗信息服务评价体系则是医疗服务诊程中, 由相互关联或相互作用要素组成的某个过程体系[4]。目前在少数发达国家, 其医疗信息服务研究领域大多徘徊在系统架构、信息本体驱动、紧急医疗服务或信息规定守则等方面, 并未有过多相关评价指标体系构建方面的研究。如Redston等[5]、Hur等[6]分别关注在线健康服务系统优化和分布式医疗信息系统可靠性问题; 中国在医疗信息服务领域的研究起步相对较晚, 但在决策机制、质量评价及实证研究方面较为成熟, 却较少关注了用户在医疗信息服务过程中的需求和感知行为体现[7], 因此以用户实际感受与认知方面为研究主体的医疗信息服务及其平台体系的搭建逐渐成为医疗信息技术研究领域的新兴热点。
本文选择顺序流程原则和灰色聚类法进行指标初选与优化, 灰色聚类适用于处理指标样本大、数据繁杂的研究, 这种方法能够保证指标选取的全面性、指标筛选与优化的科学性。以新视角(将用户感知行为视作研究整体与中心)把握用户的医疗信息服务需求和行为意向, 并构建一套完整的、科学的、系统的且适合中国医疗信息服务发展方向的评价指标体系。
用户感知是指用户在接受由企业或相关机构提供的特定产品或服务过程中对利益得失的一种感受与认知行为, 相关产品及服务是用户感知的主要目标及内容, 则用户本身是其感知主体。近年, 诸多学者多将用户感知与各领域相关服务结合, 逐渐将服务本质转移到用户本身, 如Liang等[8] 和Conceição等[9]分别以不同视角、方式, 探讨用户对信息系统的需求与满意度; 邓李君等[10]将用户感知的直接行为体现于数字图书馆影响因素研究中; 赵闯[11]和孙华[12]分别在高校图书馆学科服务评价和质量评价体系中考虑到用户感知价值的行为影响; 王巍等[13]以顾客感知视角探讨医疗信息服务评价体系。由此可知, 用户感知行为在国内医疗信息服务领域的研究仍不充分, 因此探讨用户感知层面的医疗信息服务评价体系是必要的和紧迫的。
目前Sheth、Woodruff与Philip Kotler请给出原始文献不要使用二手文献顾客感知价值模型的应用均较为广泛。Sheth从功能、社会、情感、认识和情境等5方面价值体现顾客感知价值的构成观, Woodruff从产品属性、属性偏好和结果评价三方面体现顾客感知价值的层次观, Philip Kotler则从顾客总价值和顾客总成本两方面实现顾客让渡价值观[14,15,16]。考虑基于用户感知价值的医疗信息服务评价是用户在就医全过程中对医疗信息服务的体验获得与实际感知利失之间的权衡, 同时又包含相对付出的时间、精神情感等方面的感知, 综合考虑, Philip Kotler顾客让渡价值理论模型较为适合本文的研究。
Philip Kotler顾客让渡价值模型可划分为产品价值、服务价值、人员价值、形象价值、货币成本、时间成本、体力成本与精神成本等8个维度, 深入研究并分析让渡价值模型的应用案例, 发现用户对医院所提供的医疗信息服务产品, 信息人员服务水平, 就医全过程中体力、精力消耗等方面的需求都是较为明显的, 但并没有实际体验或感知信息手段付出的货币成本, 或是某些形象价值, 如Alipour等[17]在研究医院信息系统过程中, 着重考虑人为因素、成本和时间等因素。因此本文结合王巍等[18]对顾客让渡价值的部分修改, 重构一种适用于本文的顾客让渡价值理论模型, 依据“科学性、系统性、动态性、可比性、综合性”原则构建评价体系[19], 经笔者完善后的顾客让渡价值模型分为产品价值、服务价值、人员价值、情境价值、品牌价值、冲突成本、时间+体力成本、精神成本、风险成本等9个维度, 并运用重构后的顾客让渡价值理论模型进行用户的医疗信息服务评价指标体系的构建。
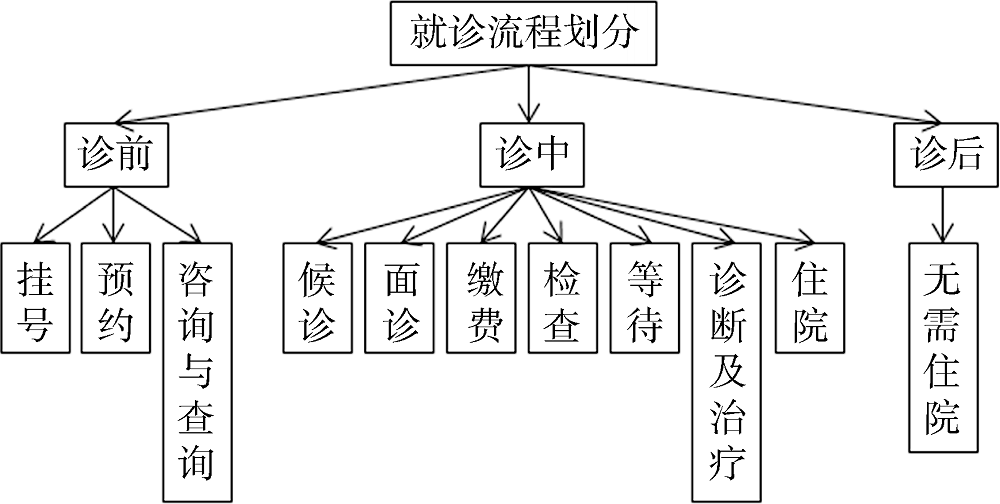
本文研究对象为医疗信息服务接受者——用户, 最终确立的评价体系是服务于医院医疗信息服务水平或质量综合评价的。基于评价目标的方向性, 以《三级综合医院评审标准实施细则》(2011版)为指标选取依据之一, 同时考虑到在医疗信息服务中, “用户、信息技术、医护人员”三者之间的交流均贯穿于用户的就诊全过程, 因此本文指标也基于文献积累和用户实际就诊应用流程进行归纳与添加。同时参考杨军弟等[20]和郑文婷等[21]学者的研究成果, 将用户在就诊过程中体验到或享受到的医疗信息服务制成相应的评价指标, 并按照诊前、诊中及诊后三个就诊流程确定本研究所需的指标及维度, 如图1所示[22]。因此所有初选指标的规划与处理均依照该标准细则、重构后的顾客感知价值模型与评价指标体系准则(目的性、全面性、可行性、稳定性和与评价方法的协调性)[23]选取, 初步确立该评价指标体系由2个层次、9个维度和80项指标构成, 如表1所示。该80项指标释义均服从用户在接受医疗信息服务过程中的感知条件。
由于用户在就诊全过程中的感知是一种动态趋势, 初步确立的指标可能部分存在归纳或选取的不确定性、重复性等弊端, 为此针对用户设计两次用户量表问卷并进行调研, 从而完善第一部分的评价指标选择, 其数据来源于吉林大学中日联谊医院。第一次量表问卷发放300份, 回收266份, 回收率88.7%; 有效问卷207份, 有效率69%。本次问卷发放时间为2016年2月中旬-2016年5月中旬, 发放地点选择在吉林省长春市吉林大学中日联谊医院、高校附近及居民区等区域, 问卷对象主要选择患者、家属及其他健康人群。其中男性为169人次, 约为56.3%; 女性为131人次, 约为43.7%。
量表设计采取李克特7级量表进行等级划分, 经过量表信度与效度分析, 检查量表问卷内在一致性与指标合理性[24]。剔除Cronbach’s α系数小于0.5的指标以检验量表的可靠性, 分别为“A7、A8、A10”、“B6、B12、B13、B14、B20”、“D5、D9、D10”和“H6”共12项, 表明这类指标题项的内部一致性信度较低, 其对应项目——总体相关系数均小于0.5, 表明其单项指标得分与总体项目总分之间的关联程度较低, 故可剔除, 则剩余68项指标进入效度分析。经量表问卷结构效度计算发现, A9、B1、B2、B17、D7和E7共6项指标的旋转因子系数小于0.5, 表明该指标题项在某一维度中的相关程度较低, 可剔除, 最终剩余62项指标进入二次量表分析。
第二次量表问卷发放260份, 回收215份, 回收率82.7%, 有效问卷180份, 有效率69.2%。本次问卷发放时间为2016年6月中旬-2016年9月中旬。考虑到第一次量表问卷多发放于高校与周围居民, 这可能导致指标筛选的方式更倾向于高等教育知识的影响, 因此第二次量表问卷的发放地点选择在吉林大学中日联谊医院、吉林大学白求恩第一医院、吉林大学第二医院及其周边居民或行人等, 问卷对象主要选择患者、家属及其他健康人群。其中男性为105人次, 约为40.4%; 女性为155人次, 约为59.6%。
由于第二次量表问卷62项指标的Cronbach’s α系数、项目-总体相关系数及旋转因子系数均大于0.5, 则仅对比两次量表问卷的9个维度Cronbach’s α系数, 如表2所示。从两次Cronbach’s α系数可知, 62项指标维度划分具有较好的信度结果, 且第二次量表问卷Cronbach’s α系数要高于第一次量表问卷Cronbach’s α, 表明上述所删除的指标题项符合客观实际, 也符合数理统计学的研究。
经过上述两轮面向用户的量表问卷调查分析, 剩余62项指标进入面向专家的指标优化环节。由于用户是医疗信息服务的主要侧重点, 通过医疗信息服务方式提升医院的医疗信息服务质量是本文最终目标, 而研究人类行为与心理变化的心理学专家, 主要讨论社会发展、问题及政策的社会学专家, 均与本文研究焦点关联甚微。于是笔者较偏向于选择信息学、临床医学与医院管理学等领域的专家, 且通过选取的9名专家(2名信息学、4名临床医学和3名医院管理学)根据指标重要程度进行等级打分, 如表3所示。计算灰色聚类矩阵, 最终形成较为完善的基于用户感知价值的医疗信息服务评价体系。
鉴于本文指标数量较多和不确定性表现, 而灰色系统对数据样本的要求不高, 适合处理大容量观测指标, 能够着重解决指标的不确定性问题[25]。灰色聚类是以灰色系统理论为基准, 依据各项指标关联度矩阵进行观测样本的分类[26,27]。设分析系统
$R=\left[ \begin{matrix} {{\varepsilon }_{11}} & {{\varepsilon }_{12}} & ... & {{\varepsilon }_{1m}} \\ {} & {{\varepsilon }_{22}} & ... & {{\varepsilon }_{2m}} \\ {} & {} & \ddots & \vdots \\ {} & {} & {} & {{\varepsilon }_{mm}} \\\end{matrix} \right]$ (1)
其中, ${{\varepsilon }_{ii}}=1,\ i=1,2,\cdot \cdot \cdot ,m$。选取适当关联矩阵临界值$r\in (0,1]$, 挑选出${{\varepsilon }_{ii}}\ge r\ (i\ne j)$的指标, 此时可视为${{X}_{i}}$与${{X}_{j}}$拥有相同属性, 则可将其归纳为同类别。由于篇幅限制, 本文将指标关联矩阵拆分成6块关联矩阵:${{R}_{\mathrm{(}1\mathrm{)}}}$、${{R}_{\mathrm{(}2\mathrm{)}}}$、${{R}_{\mathrm{(}3\mathrm{)}}}$、${{R}_{\mathrm{(}4\mathrm{)}}}$、${{R}_{\mathrm{(}5\mathrm{)}}}$和${{R}_{\mathrm{(}6\mathrm{)}}}$。
${{R}_{\mathrm{(1)}}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.81 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.77 \\ 0.87 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.65 \\ 0.58 \\ 0.71 \\ \begin{matrix} 1.00 \\ {} \\ {} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.70 \\ 0.89 \\ 0.66 \\ \begin{matrix} 0.81 \\ 1.00 \\ {} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.79 \\ 0.73 \\ 0.62 \\ \begin{matrix} 0.63 \\ 0.70 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
${{R}_{(2)}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \text{0}\text{.80} \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \text{0}\text{.66} \\ 0.68 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} \text{0}\text{.91} \\ 0.61 \\ 0.58 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.61 \\ 0.70 \\ 0.74 \\ \begin{matrix} 0.80 \\ \text{1}\text{.00} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.71 \\ 0.76 \\ 0.74 \\ \begin{matrix} 0.66 \\ \text{0}\text{.72} \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.98 \\ 0.77 \\ 0.66 \\ \begin{matrix} 0.65 \\ \text{0}\text{.75} \\ 0.89 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.87 \\ 0.95 \\ 0.70 \\ \begin{matrix} 0.67 \\ 0.78 \\ 0.69 \\ \begin{matrix} 0.72 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.69 \\ 0.54 \\ 0.77 \\ \begin{matrix} 0.66 \\ 0.73 \\ 0.78 \\ \begin{matrix} 0.94 \\ 0.74 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.70 \\ 0.72 \\ 0.62 \\ \begin{matrix} 0.56 \\ \text{0}\text{.61} \\ \text{0}\text{.69} \\ \begin{matrix} \text{0}\text{.76} \\ \text{0}\text{.72} \\ \text{0}\text{.70} \\ \begin{matrix} \text{1}\text{.00} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.59 \\ 0.65 \\ 0.65 \\ \begin{matrix} 0.66 \\ 0.62 \\ 0.59 \\ \begin{matrix} 0.59 \\ 0.60 \\ 0.68 \\ \begin{matrix} 0.57 \\ 1.00 \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.72 \\ 0.76 \\ 0.66 \\ \begin{matrix} 0.58 \\ 0.60 \\ 0.60 \\ \begin{matrix} 0.70 \\ 0.68 \\ 0.62 \\ \begin{matrix} 0.91 \\ 0.88 \\ 1.00 \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.64 \\ 0.72 \\ 0.63 \\ \begin{matrix} 0.73 \\ 0.68 \\ 0.61 \\ \begin{matrix} 0.73 \\ 0.75 \\ 0.63 \\ \begin{matrix} 0.89 \\ 0.68 \\ 0.65 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
${{R}_{\mathrm{(}3\mathrm{)}}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.95 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.60 \\ 0.51 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.87 \\ 0.91 \\ 0.94 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.67 \\ 0.98 \\ 0.89 \\ \begin{matrix} 0.77 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.71 \\ 0.65 \\ 0.73 \\ \begin{matrix} 0.70 \\ 0.88 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.75 \\ 0.50 \\ 0.62 \\ \begin{matrix} 0.75 \\ 0.79 \\ 0.50 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.67 \\ 0.64 \\ 0.66 \\ \begin{matrix} 0.70 \\ 0.69 \\ 0.68 \\ \begin{matrix} 0.63 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.68 \\ 0.62 \\ 0.69 \\ \begin{matrix} 0.73 \\ 0.69 \\ 0.70 \\ \begin{matrix} 0.66 \\ 0.68 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.73 \\ 0.67 \\ 0.65 \\ \begin{matrix} 0.75 \\ 0.72 \\ 0.72 \\ \begin{matrix} 0.76 \\ 0.67 \\ 0.84 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.71 \\ 0.71 \\ 0.64 \\ \begin{matrix} 0.53 \\ 0.69 \\ 0.70 \\ \begin{matrix} 0.65 \\ 0.87 \\ 0.81 \\ \begin{matrix} 0.93 \\ 1.00 \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.78 \\ 0.74 \\ 0.67 \\ \begin{matrix} 0.68 \\ 0.69 \\ 0.77 \\ \begin{matrix} 0.56 \\ 0.87 \\ 0.61 \\ \begin{matrix} 0.73 \\ 0.63 \\ 1.00 \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.71 \\ 0.67 \\ 0.66 \\ \begin{matrix} 0.68 \\ 0.72 \\ 0.65 \\ \begin{matrix} 0.65 \\ 0.62 \\ 0.71 \\ \begin{matrix} 0.79 \\ 0.71 \\ 0.61 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
${{R}_{\mathrm{(}4\mathrm{)}}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.67 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.93 \\ 0.59 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.71 \\ 0.84 \\ 0.91 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.83 \\ 0.87 \\ 0.67 \\ \begin{matrix} 0.71 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.88 \\ 0.74 \\ 0.89 \\ \begin{matrix} 0.71 \\ 0.67 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.76 \\ 0.68 \\ 0.62 \\ \begin{matrix} 0.73 \\ 0.54 \\ 0.76 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.64 \\ 0.57 \\ 0.62 \\ \begin{matrix} 0.67 \\ 0.68 \\ 0.66 \\ \begin{matrix} 0.91 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.60 \\ 0.73 \\ 0.61 \\ \begin{matrix} 0.76 \\ 0.55 \\ 0.71 \\ \begin{matrix} 0.85 \\ 0.62 \\ 1.00 \\ \begin{matrix} {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.62 \\ 0.59 \\ 0.65 \\ \begin{matrix} 0.54 \\ 0.57 \\ 0.55 \\ \begin{matrix} 0.58 \\ 0.84 \\ 0.55 \\ \begin{matrix} 1.00 \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.76 \\ 0.51 \\ 0.58 \\ \begin{matrix} 0.74 \\ 0.57 \\ 0.64 \\ \begin{matrix} 0.72 \\ 0.92 \\ 0.69 \\ \begin{matrix} 0.57 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
${{R}_{\mathrm{(}5\mathrm{)}}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.64 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.76 \\ 0.86 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.92 \\ 0.69 \\ 0.69 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.82 \\ 0.71 \\ 0.98 \\ \begin{matrix} 0.73 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.71 \\ 0.66 \\ 0.75 \\ \begin{matrix} 0.61 \\ 0.76 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.63 \\ 0.60 \\ 0.66 \\ \begin{matrix} 0.78 \\ 0.78 \\ 0.71 \\ \begin{matrix} 1.00 \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.75 \\ 0.70 \\ 0.88 \\ \begin{matrix} 0.88 \\ 0.77 \\ 0.75 \\ \begin{matrix} 0.63 \\ 1.00 \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.61 \\ 0.73 \\ 0.66 \\ \begin{matrix} 0.73 \\ 0.88 \\ 0.79 \\ \begin{matrix} 0.70 \\ 0.66 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
${{R}_{\mathrm{(}6\mathrm{)}}}=\left[ \begin{matrix} \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.64 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.89 \\ 0.92 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.87 \\ 0.75 \\ 0.72 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.64 \\ 0.74 \\ 0.68 \\ \begin{matrix} 0.65 \\ 1.00 \\ {} \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.90 \\ 0.72 \\ 0.68 \\ \begin{matrix} 0.74 \\ 0.86 \\ 1.00 \\ \begin{matrix} {} \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} \begin{matrix} 0.87 \\ 0.46 \\ 0.57 \\ \begin{matrix} 0.55 \\ 0.59 \\ 0.87 \\ \begin{matrix} 1.00 \\ {} \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.63 \\ 0.62 \\ 0.80 \\ \begin{matrix} 0.54 \\ 0.69 \\ 0.79 \\ \begin{matrix} 0.52 \\ 1.00 \\ {} \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.58 \\ 0.58 \\ 0.64 \\ \begin{matrix} 0.55 \\ 0.64 \\ 0.53 \\ \begin{matrix} 0.76 \\ 0.85 \\ 1.00 \\ {} \\\end{matrix} \\\end{matrix} \\\end{matrix} & \begin{matrix} 0.57 \\ 0.45 \\ 0.59 \\ \begin{matrix} 0.53 \\ 0.51 \\ 0.48 \\ \begin{matrix} 0.77 \\ 0.88 \\ 0.91 \\ 1.00 \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \\\end{matrix} \right]$
通过对比6个关联矩阵, 取临界值$r=0.8$, 可发现服务价值中“B5信息知晓查询平台服务”、情境价值中“D1医疗设备摆放位置”和“D11信息服务承诺可靠性”、时间+体力成本中“G6药品信息取获时间”与任一指标的灰色关联度均小于0.8, 因此可剔除此4项指标, 原维度的剩余指标位置均无变化, 继而可验证本文指标划分与归类的合理性、科学性。则剩余58项指标共分为9类, 计算其权重, 如表4所示。
$\left\{ \left. {{A}_{1}},{{A}_{2}},{{A}_{3}},{{A}_{4}},{{A}_{5}},{{A}_{6}} \right\} \right.$、$\left\{ {{B}_{3}},{{B}_{4}},{{B}_{7}},{{B}_{8}},{{B}_{9}},{{B}_{10}},{{B}_{11}}, \right.$ $\left. {{B}_{15}},{{B}_{16}},{{B}_{18}},{{B}_{19}},{{B}_{21}} \right\}$、$\left\{ \left. {{C}_{1}},{{C}_{2}},{{C}_{3}},{{C}_{4}},{{C}_{5}},{{C}_{6}} \right\} \right.$、$\left\{ {{D}_{2}},{{D}_{3}}, \right.$ ${{D}_{4}},\left. {{D}_{6}},{{D}_{8}} \right\}$、x$\left\{ \left. {{E}_{1}},{{E}_{2}},{{E}_{3}},{{E}_{4}},{{E}_{5}},{{E}_{6}} \right\} \right.$、$\left\{ {{F}_{1}},{{F}_{2}},{{F}_{3}}, \right.$$\left. {{F}_{4}},{{F}_{5}} \right\}$、$\left\{ \left. {{G}_{1}},{{G}_{2}},{{G}_{3}},{{G}_{4}},{{G}_{5}},{{G}_{7}},{{G}_{8}},{{G}_{9}} \right\} \right.$、$\left\{ {{H}_{1}},{{H}_{2}},{{H}_{3}},{{H}_{4}},{{H}_{5}}, \right.$ $\left. {{H}_{7}},{{H}_{8}} \right\}$和$\left\{ \left. {{I}_{1}},{{I}_{2}},{{I}_{3}} \right\} \right.$。
通过权重计算结果可知, 服务价值维度权重比例最大为0.2059, 风险成本维度的权重比例最小为0.0405, 导致这种权重排序的主要原因可能是由于本次调研区域局限于吉林省, 而不同省份之间文化差异与保护知识的意识程度均有可能是潜在的影响因素, 因此未来调研区域将扩展至北京、辽宁省及部分经济文化发展较快的省市区域, 并进一步深入调查研究; 其次是精神成本中“H7结果信息咨询沟通压力”的权重值最大为0.0201, 用户在实际就医中接受信息服务时, 往往由于初次接触信息处理设备, 会出现一种无从获知操作方式的负面抵触情绪, 医院医护人员及导诊人员的分配情况或回复不及时等皆是影响用户信息就医满意程度的直接因素; 此外, 情境价值中“D6患者网络数据安全”和品牌价值中“E4医疗信息打印设备出图质量”的权重值位列第二且均为0.0200, 出现此调研结果可能是由于当今是大数据互联共通的时代, 用户实际生活中往往会频繁遭遇不明电话的侵扰、推销等现象, 因此用户更为看重医院对于自身病情信息及个人基本信息的保护情况, 同时也关注医院所提供的医疗信息设备是否具有良好的性能且能够满足自身的就医需求; 在权重比例中最小的是精神成本中“H8信息设备权威性担忧”, 仅为0.0103, 在实际调研走访中, 绝大多数用户对于医疗信息设备的权威性均没有过于在意, 这可能是由于本次调研群体的文化层次或工作领域所导致的, 因此未来调研会深入观测群体的基本文化教育及工作信息。
本文提出一种面向用户、医疗信息服务人员及医疗信息产品的顾客感知价值理论模型的新框架, 从产品价值、服务价值、人员价值、情境价值、品牌价值、冲突成本、时间+体力成本、精神成本和风险成本等9个方面提出一套基于用户感知价值的医疗信息服务评价体系, 并用灰色聚类验证该评价体系的科学性与确定性。研究表明, 吉林省用户对医疗信息服务中服务价值与人员价值需求与期望较高, 相对来说对情境价值和风险成本的担忧较小; 此外在所有指标中, 用户更为在意的是“H7结果信息咨询沟通压力”, 也就是说医患沟通仍然是该省医院待解决的主要问题, 因此配备信息服务的医院可依据本文提出的评价体系, 适当结合当地医疗水平有效地实现服务质量的提升。该评价体系较一般评价手段具有更全面、更系统、更科学合理的优势, 能够在一定程度上帮助以信息手段服务医疗用户的医院快速发现影响用户不同就诊阶段的感知因素, 并有针对性地提升相关指标的服务效果, 为日后融入信息技术的医疗研究提供借鉴尽量不要在结语初引用。
李健: 提出论文框架与思路, 论文修改及最终版本修订;
王明月: 数据处理、统计分析与挖掘;
许路明: 采集数据, 整理文献;
田英春: 起草论文, 搜集数据。
所有作者声明不存在利益冲突关系。
支撑数据由作者自存储, E-mail:984469122@qq.com。
[1] 李健, 王明月. 第一次用户调查问卷.doc. 第一次用户调查问卷.
[2] 李健, 王明月. 第二次用户调查问卷.doc. 第二次用户调查问卷.
[3] 李健, 王明月. dafenbiao.xls. 专家打分表.
[4] 李健, 王明月. daima.doc. 灰色聚类代码.
| [1] |
远程医疗是利用远程通信技术和信息技术,面向区域范围内的患者、医务工作者、医疗机构等提供的一种新型医疗服务方式,欧美许多发达国家在远程医疗服务取得了突破性进展,积累了丰富的经验.近十年,我国远程医疗服务也逐步开展并取得了一定的成绩,但相比欧美发达国家仍有较大的提升空间.本文在了解欧美发达国家远程医疗服务的基础上,针对我国远程医疗服务现状,提出可供参考的建议.
URL
[本文引用:1]
|
| [2] |
“互联网+医疗”为医疗服务模式变革提供了新的思路,O2O医疗服务具有线上线下一体化融合的特点,成为互联网+医疗的具体体现和突破口.研究构建基于云平台的O2O医疗服务体系架构,并分析其服务类型,在此基础上介绍了目前O2O医疗服务的典型应用,最后探讨了我国发展O2O医疗服务面临的问题及对策.
URL
[本文引用:1]
|
| [3] |
[本文引用:1]
|
| [4] |
提出了要建立医疗服务评价指标体系,需建立医疗服务质量评价系统以及构建医疗服务质量评价模型图。同时指出医疗服务质量指标确定应遵循独立性、全面性、目标导向、重要性以及实用性和可操作性等原则。并且在实施医疗服务评价指标体系时要明确关键点,领导重视是关键,全员参与是动力,规范有序是前提,信息管理是依据,严格考核是助力。
|
| [5] |
Findings support the growing recognition that online health information can contribute to the resolution of embarrassing medical problems, but demonstrate that outcomes may vary with medical problem type. The results indicate that building data collection into online information provision can help to refine and focus health information for online users.
|
| [6] |
Medical information systems facilitate ambulatory patient care, and increase safer and more intelligent diagnostic and therapeutic capabilities through automated interoperability among distributed medical devices. In modern medical information systems, dependability is one of the most important factors for patient safety in the presence of delayed or lost system alarm and data streams due to the intermittent medical device network connection or failure. In addition, since the medical information need to be frequently audited by many human operators as well as the automated medical devices, secure access control is another pivotal factor for patient privacy and data confidentiality against inside or outside adversaries. In this study, we propose a dependable and secure access policy enforcement scheme for disruption-tolerant medical information systems. The proposed scheme exploits the external storage node operated by the device controller, which enables reliable communications between medical devices. Fine-grained data access control is also achieved, while the key escrow problem is resolved such that any curious device controller or key generation center cannot decrypt the private medical data of patients. The proposed scheme allows the device controller to partially decrypt the encrypted medical information for the authorized receivers with their corresponding attributes without leaking any confidential information to it. Thus, computational efficiency at the medical devices is also enhanced by enabling the medical devices to delegate most laborious tasks of decryption to the device controller.
|
| [7] |
【目的/意义】在线健康社区逐渐成为用户获取医疗信息服务的重要途径。【方法/过程】基于感知价值理论,构建在线健康社区用户信息服务使用意愿影响因素模型,采用问卷调查方法收集数据,利用Smart PLS 3.0工具检验提出的假设,并进一步探究性别对影响效果的调节作用。【结果/结论】研究结果表明:社会支持、成就需要和感知信任对用户使用意愿具有显著地正向影响,感知风险对用户使用意愿具有显著地负向影响,对于不同性别用户,各变量的影响效果有一定的差异。
URL
[本文引用:1]
|
| [8] |
The relationship between a doctor and a patient plays an important role in patient satisfaction with health-care services. It has become an important and contentious issue in China’s health-care reform. This study uses service fairness as a theoretical lens to investigate the influence an implementation of a patient-accessible hospital information system (HIS) has on doctor–patient relationships and patient satisfaction. We developed a research model that relates patient-accessible HIS implementation with perception of service fairness, doctor–patient relationships, and patient satisfaction. Data were collected from patients in one of the biggest hospitals in East China that has implemented patient-accessible HIS. Results of the study show that patient-accessible HIS promotes patients’ perception of service fairness, improves doctor–patient relationships, and increases patient satisfaction.
|
| [9] |
|
| [10] |
<p>用户价值感知直接体现用户对图书馆所提供的资源和服务的主观认知,而数字资源丰裕度、新技术运用、资源整合力度等诸多方面的原因都能对用户价值感知形成影响。实验以数字资源影响用户感知价值的多种因素为因子,利用SPSS分析数字资源影响用户感知价值的重要因素,提出促进高校图书馆数字资源的合理建设、科学管理和高效利用的对策。</p>
|
| [11] |
本文将顾客感知价值理论应用到高校图书馆学科服务评价研究中,结合SERVQUAL量表与LibQUAL+模型,提出学科服务评价的SUB-SERVQUAL评价模型,以评价图书馆学科服务状况,并详细介绍了评价体系与评价方法。
URL
[本文引用:1]
|
| [12] |
评价高校图书馆信息服务的质量,是促进图书馆工作发展重要环节,通过对信息用户感知服务,建立图书馆信息服务评价体系,更好地强化图书馆信息资源科学配置,提高图书馆"硬质量"和"软质量"建设,促进图书馆服务教学科研。
|
| [13] |
本文以问卷调查的形式获取影响用户感知价值的医疗信息服务的因素,并以用户感知价值为导向,通过SPSS统计软件及文献回顾对当前医疗信息服务项目进行整理、总结,最终从总价值和总成本两个维度共8个评价指标的角度构建了医疗信息服务项目的感知价值指标体系,以期为后续提高医疗信息服务质量的研究提供参考.本文的研究结果可用于建设和完善医疗信息服务项目,评价医疗信息服务质量.
|
| [14] |
No abstract is available for this item.
|
| [15] |
|
| [16] |
Examines how widely held country images affect attitudes towards a country's products and services and ability to attract investment, businesses and tourists. Role of brands in creating product differentiation; Impact of country names on attitudes toward products; Tasks of country brand management.
|
| [17] |
Abstract INTRODUCTION: After implementation, evaluation of hospital information systems (HISs) is critical to ensure the fulfillment of the system goals. This study aimed to assess the success or failure of HISs in public hospitals affiliated with Zahedan University of Medical Sciences. MATERIALS AND METHODS: A cross-sectional descriptive and analytic study was performed in 2016. The study population comprised IT and HIS authorities and hospital information system users. The sample consisted of 468 participants. The data were collected using two questionnaires and analyzed with the SPSS software using descriptive and analytical statistics. RESULTS: The mean score of functional, behavioral, ethical, organizational, cultural and educational factors from the users' perspective was 3.1400±0.66, 2.9700± 0.60, 3.3900±0.70, 2.9600±0.642, 3.0900±0.63, and 2.9500±0.74, respectively. The mean score of organizational, behavioral, cultural, technological, educational and legal factors from IT and HIS authorities' perspective was 3.5100±0.54, 3.3500±0.45, 2.7500±0.61, 3.5800±0.32, and 3.9600±0.59, respectively. CONCLUSIONS: The evaluated hospital information systems were considered relatively successful in terms of functional, ethical, and cultural factors but were considered as a relative failure in terms of behavioral, organizational, and educational factors form the users' perspective. Only the legal factor showed success, while organizational, behavioral, technical and educational factors showed relative success and the cultural factor showed relative failure from HIS and IT authorities' perspective. Therefore, assessing the users' needs before implementing the system, involving them in various stages of implementation, training them, and improving their computer skills seem to be necessary to achieve a better level of system success. Copyright 0008 2017 Elsevier B.V. All rights reserved.
|
| [18] |
在系统梳理感知价值相关研究成果的基础上,从信息服务领域的特性出发,分析用户感知价值研究中所涉及的基本问题,消除其界定上的模糊性,识别构成用户感知价值的驱动因素,旨在为预测信息用户需求和行为方式、持续提高用户满意度、实现用户需求为导向的信息服务目标提供理论及方法支持。
URL
[本文引用:1]
|
| [19] |
在当前教育改革力度不断加大的背景下,高校的财务管理环境也越来越复杂,财务管理的复杂性以及管理难度都呈现出逐渐上升的趋势。在这种情况下,高校要想提高财务管理的有效性,必须要根据实际情况构建财务绩效评价体系。本文结合笔者的工作经验和理解,就高校财务绩效评价体系的有效构建阐述一下自己的观点,以供参考。
URL
[本文引用:1]
|
| [20] |
旨在了解北京市三甲医院门诊就诊相关信息服务方式现状,主要采用观察法进行资料收集。结果提示,医院根据就诊不同环节信息内容的差异设置了多样化的信息服务方式,包括传统方式和现代信息技术的应用。三甲医院应相互学习和借鉴,并结合患者的需求和习惯,使信息服务内容和方式更好地结合,进一步提升门诊信息服务的效果。
|
| [21] |
当今社会多元化的发展,对综合医院门诊服务的内容及服务形式也提出了更高的要求。文章总结了在信息化建设的基础上门诊流程的优化升级,包括各类诊前自助、诊间及诊后服务,创建了一个"以患者为中心"的门诊就医流程,为患者提供了方便快捷的就医环境。同时也指出制度保障、精细化管理和全方面宣传引导是流程优化的运行保障。但不免也继续存在或出现一些问题,如号贩子倒号问题、诊间加号秩序问题和患者检查多次往返等问题,还需在理论上进一步研究,在实践中进一步改善,从而使患者感受到更加方便快捷的医疗服务,真正做到"以病人为中心"服务。
|
| [22] |
目的利用互联网信息技术开展医院门诊业务流程的优化和再造,提高工作效率和就诊者满意度。方法收集门诊就诊流程优化前后我院的门诊流程环节、门诊量和就诊者等待时间及患者满意度调查记录,对门诊就诊流程优化前后就诊环节、就诊排队、门诊服务站点、就诊秩序、信息传输进行对比分析。结果门诊流程优化后,门诊在诊人次逐年递增至137%,就诊等待时间平均缩短20 min,患者满意度逐年提升。结论利用信息技术优化门诊流程,对改善门诊就诊环境,提高门诊工作效率、提升门诊服务效能,保证服务质量,提高就诊者满意度具有显著的效果。
|
| [23] |
介绍了综合评价的逻辑过程及指标体系的建立在综合评价中的重要地位,讨论了指标体系初建、筛选和结构优化的研究现状、运用的基本方法及方法的优劣,分析了多属性综合评价指标体系理论的发展趋势。
|
| [24] |
消费养老是将消费增值的价值以养老保障的形式回馈给消费者,它作为一种新型的养老方式,具有传统养老方式没有的优势。然而,在实际推行中会涉及到企业、银行、保险机构等多方面的配合与协作。针对这种新型养老方式的社会认知程度设计基于李克特式的量表,并对调查问卷进行初步统计分析,提出安全性、遗产观念等影响选择该方式的主要因素。
|
| [25] |
文章基于情报3.0背景下科技情报服务能力的总体架构及内容,研究了科技情报服务能力评价思路,并借助调查法与统计方法、德尔菲法、灰色数学统计法、层次分析法具体论证了情报资源保障能力、情报交互能力、情报分析判断能力和情报协同服务能力的一级和二级评价指标,设计了指标权重,提出科技情报服务能力的评价指标体系。
|
| [26] |
现如今企业信息化发展非常迅速,相应的ERP人才需求激增。如何科学、客观的评判学生的ERP能力是重中之重。本文研究的重点就是通过灰色关联聚类,分析学生的ERP能力指标,把相同或相似的指标进行归类,使复杂的指标体系简单化,达到实用可靠的目的。
URL
[本文引用:1]
|
| [27] |
服务性是图书馆的本质属性之一,服务工作的好坏,服务质量的高低,都直接决定着一个图书馆的整体水平和实力.从目前国内外的研究情况来看,有关高校图书馆服务质量评价理论与方法的研究基本围绕单一因素来展开,如图书馆基础条件的建设、读者感受或馆员对图书馆氛围与多样化的满意度等方面.但图书馆服务质量评价是一个综合评价体系,对某一因素或某些因素进行的评价具有片面性,不能全面考证图书馆的服务质量.因此,文章建立一套包含条件、读者、馆员等主客观因素的图书馆服务质量评价体系,并确定每个因素在图书馆服务中的重要程度,进行实证研究.构建针对高校图书馆的粗集与自回归移动平均相结合的评价模型,应用到我国高校图书馆评价当中.实证研究结果表明,通过引入粗集理论可有效约简冗余数据信息,使得模型的可靠性、合理性和科学性得到更好保证,也提高了模型的分类效果,具有良好的学习推广能力和评价能力.
|



{kind=link}
{kind=link}